Juliet’s HBAC after Inverted T
I wrote my first two birth stories within 24 hours of birth and felt the pull to get this one out quickly as well. I think it’s probably because I’m riding birth hormone highs and it’s all fresh or it’s because each birth has been better than the last so I’m more anxious to share. Either way, I’ve had a ton of requests for this birth story and I’ve always known that I would write it so, 16 hours later, here goes…
To really understand Juliet’s birth story it helps to know my history and that starts with her brother Graham’s story. He was my first, almost 9 years earlier and was born after a difficult labor that ended in a c section with an inverted T incision rather than the typical low transverse or “bikini cut” that most c sections are. We both had a lot of emotional and physical birth trauma. I went on to have a HBAC (home vaginal birth after cesarean) with my daughter two years later which is 6.5 years ago. I divorced later that year and wasn’t sure if I’d have more babies. I’d hoped I would, I didn’t feel done, I was only 31 at the time but I didn’t know what the future held.
I met my husband 5 years later and we married in September of 2015. We discussed having a baby but age was a factor. While I don’t really think advanced maternal age is an issue at just turning 37, my husband is 11 years older than me so starting over with a baby was a big deal. After 6 months of marriage, 2 months after an IUD removal and not actively trying to conceive (we were ovulation testing since I didn’t know what my cycle would look like after the IUD) I was pregnant anyway so we immediately switched gears from “do we want a baby?” to “we are having a baby!!!!!” Sometimes it’s just meant to be.


I started this pregnancy much healthier than my previous two. After my second baby I lost 85lbs and had become a marathon runner. I also eat a very clean diet 90% of the time. Health and wellness are important to our family so even though I was 6 years older, I felt better than I did in the previous two pregnancies. The first trimester morning sickness was a drag but passed. I quickly figured out my birth options, which were few due to my previous inverted T incision c section. The standard of care for obstetrical maternity care is a c section at 37 weeks with this type of scar. Because I’d already had a VBAC that wasn’t an option for me, I intended to VBAC again. I have a “proven scar” and “proven pelvis” and my previous VBAC, though difficult, was a much better choice than a repeat cesarean. Tony, my husband, was already on board with a home birth and we are very like minded so I had his support and I knew without a doubt that we would be a cohesive team through the pregnancy and birth.
The home birth midwives in CO can’t accept VBAC clients that have any kind of scar other than the bikini cut. There was one OB in our town of half a million people that would accept me as a patient but having already had a home birth I struggled with that idea. I reached out to a midwife that I’d talked to when I was looking for a helper for my first VBAC. I lived in Korea for my first VBAC and she had traveled there twice to help another family. Birthy people blog so I heard about her 7 years ago. I didn’t hire her to come to Korea because I ended up finding local help but when I reached out to her for this birth she agreed to travel from Montana to come help us. We had that conversation at 6 weeks pregnant. I’m a planner. Plus I just wanted to gestate in peace and knowing that was covered sealed the deal. I did have some OB prenatal care in the event that we needed to transfer during birth. I figured an established patient record would help ensure a smooth transition if that happened. I wasn’t concerned about transferring too much though. I’ve just had a history of very long hard labors so I like to cover bases. My last prenatal visit there was at 37 weeks. This pregnancy was almost text book perfect and despite getting really tired the last month or so, it was really enjoyable. I’ll miss it as much as I’m glad she’s here.
So, the big debate on WHEN the baby would come, boy or girl, size, length of labor and how long I’d push was ongoing. My first pregnancy was 41 weeks and 2 days and labor was 52 hours, 8lbs 5oz, c/s. The second was 41 weeks and 4 days, 40 hours labor plus 4 hours of pushing and 9lbs 3oz. One had a 15 inch head and the second 15.5. Birth average is 13.75….
Tony, who is a Physical Therapist with extensive visceral therapy training, had been treating my abdomen pretty much since we met and a lot after my IUD removal. I had scarring from my previous c/s and also from a diastasis recti repair (ab muscle separation, mine was really bad) 5 years earlier. Treating the scar tissue would help me have a better birth. Treating my pelvis and making sure I had good alignment was also a part of that. He took excellent care of me and between that and not gaining much weight I hardly had any aches and pains. It was a nice change from the 70 and 55lbs weight gains before and the misery I felt daily. I believe it’s also why Juliet engaged prior to labor when my first two did not. I had a baby ready pelvis, no scar tissue holding her back and abs tight enough to hold her in place in a good position. By 38 weeks she moved down and I felt like I had a bowling ball between my legs. The pressure on my cervix was intense. I’d never experienced that before. She was also in an optimal birth position, no sunny side up or funky stuff like my other two. They were never lower than a -3 station because of their presentations and big heads. Labor was hard with them because of the molding required. I never had a vaginal exam in pregnancy with Juliet so I don’t know how low she was prior to labor but we figured -1 or even 0 as it got closer.
On December 14th I started having Braxton Hicks contractions off and on all day. I never noticed them in my other pregnancies and not really in this one either until then. They’d just get really tight and come and go. On December 15th at 39 weeks and 6 days, after a crappy night’s sleep because I just couldn’t get comfortable (no ctx though) and being cranky, we got up at our usual 6:30am. I made my family breakfast like I do every day and kept having those BH contractions once I was up and moving. I went to the bathroom around 8:30am and had bloody show. Another first, I’d never had it prior to active (and hours) of labor. Within the next hour the contractions were more than BH but not painful. I could just feel then annoying my cervix a little. I went to the bathroom again and had some mucous plug come out with more show. I’d also never had plug before active labor so I wasn’t sure what it meant for me. I told Tony, who was about to leave to go work a clinic he works at one half day a week (otherwise he’d be home at our private practice). I could tell he was excited that things were happening and that he didn’t want to go but I assured him it was just warm up and it would be a while if anything happened and it could just fizzle out anyway. I decided to skip my morning walk and take a bath. I guess I was testing the contractions and figured if it was just BH that a bath would make them stop. Tony left and I was in the bath at 8:45am.
I spent about 45 minutes in the tub. I didn’t notice any contractions while I was in there. I got out and they came back, still annoying my cervix but not painful. I posted a 40 week belly picture on FB because I figured if it was real that this was the last chance. I went downstairs to get my dog wash lady situated and my midwife was at the kitchen table. This was at 9:40am. She’d arrived three days earlier from Montana. She came earlier than I’d asked because of bad weather potential and midwife intuition. I was convinced that the baby wouldn’t be here until closer to 41 weeks but was glad she was here, it’s a long drive and it was nice to spend some time with her. She and I chatted, I ate again and I told her about the contractions, show and plug. We timed a few and they were coming regularly at 3-5 minutes apart. My last labor started hard and furious so even though these contractions were close they were only about 30 seconds long and not painful. I decided to try to take a nap.

39w6d
I put on my Hypnobabies fear clearing track and didn’t sleep. The contractions were coming easily 3 minutes apart and while still not painful were more than just BH. The cervical pressure was more intense. I texted Tony an update. I FB messaged some friends. I decided to get up and put on a full face of makeup. While I was doing that I realized I was in real labor. It was early labor, I could still walk and talk through contractions but it was happening. Tony called and we talked about what was happening and decided he should still go run errands he’d planned. I just knew it would be a while before things ramped up.
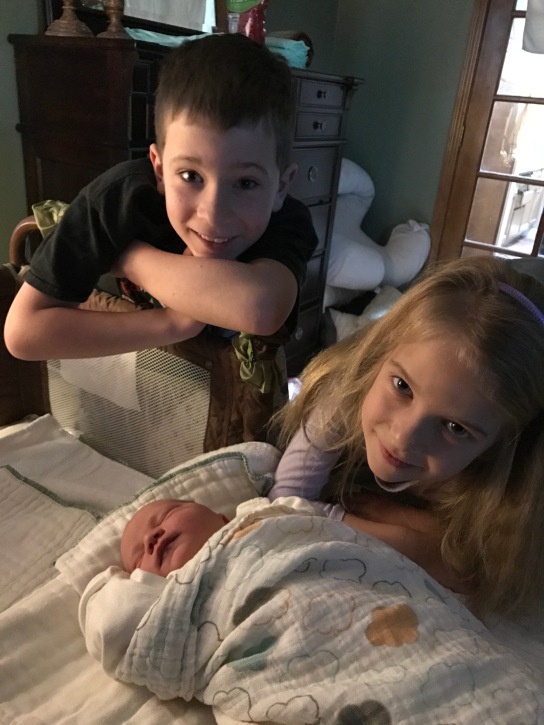
Tony got home at 1pm. I was so glad, I was fine but just wanted him home. We ate some lunch and chatted. The contractions were still consistently coming every 3-4 minutes. I decided to try once more to take a nap. That wasn’t happening, I couldn’t handle laying down anymore. It was getting too intense. I decided to put on my labor clothes: my black Bravado nursing bra and my night gown. We hung out in our upstairs office area and I put my Hypnobabies Easy first stage labor track in my ear. Tony ran around the house getting a few things done and went to meet Graham and Stella walking home from school. For me, getting them home was the last big thing that needed to happen. Tony told them the baby was coming soon and they both kind of sheepishly came upstairs to see me. We had talked about what would happen, how the baby would come out and watched birth videos but at 6 and 8 they were still a bit nervous. We hugged and kissed and took pictures of my last day as a mama of 2 and then they happily ran off to rot their brains on their tablets.


The contractions were picking up in intensity and I had to concentrate through them. I sat on my birth ball for a while but the pressure in my crotch was too much. I kneeled on the floor and rested my upper body on the ball. We had music playing and a song came on that made me cry. Tony just sang and rubbed my back. I should have recognized that was labor really picking up speed. I kept having to pee a lot and the contractions were coming 3 minutes apart. In my head there was still a lot of time ahead of us. I started standing for the contractions. It was the most comfortable position, leaning over my desk and standing. Tony had gone downstairs to get me some water and the midwife asked how things were. We were happy with our privacy and she was respecting that. She told him what kind of noises to listen for from me and to come get her if I do xyz. He told her I wasn’t making noise and we haven’t even filled up the birth pool yet. She told him the baby didn’t care. We all got a good laugh.
When he came back up stairs we decided to go ahead and fill the pool. I wasn’t sure I was ready to get in just yet but I knew it would take a while to fill. The water pressure just wasn’t cutting it though and it was coming out a quarter of what it should have. My contractions really seemed to increase in intensity but weren’t super long but I was really starting to work and breath through them. I had 3-4 four that instead of kind of standing and rocking my hips through them and lightly squatting into them, that I came up on my toes and bared down against them. I didn’t think I was pushing and I wasn’t have the overwhelming pushing contractions that I’d had last time. I was just trying to make it easier to get through.


I
I then felt something….
I felt something in my vagina. It didn’t make sense to me. I put two fingers in and felt something. I wiggled it back and forth between my two fingers. It was kind of long and thin feeling but not like the umbilical cord but not like a bulging amniotic sac of water either. Tony was still messing with the pool and I told him I felt something to go get Ollie (the MW). He was like “HUH?!” Really same as me but he RAN down the stairs and Ollie was up the stairs before I even knew it. She couldn’t see from my standing/bending over position so we went to my bed. Tony ran and turned on the bath tub assuming that I’d just get in there if something was coming out. I got in the bed and Ollie looked and it was the water bag coming out in front of the baby. At that moment I had a giant urge to push, that I hadn’t previously had and in 2-3 pushed it came out. Ollie tore a hole in it because the head was just behind it. Tony said “Oh my God baby you’re doing it!” After the bag came out I didn’t want to push the baby out. I wasn’t ready. I wasn’t prepared. It was happening fast, I didn’t realize it was coming and I wasn’t in the water. I did NOT want to be in the bed. I did NOT want to be reclining back with the MW and my husband watching. I wanted to be on my knees in the water so Tony could catch the baby. How did I go from thinking “This baby will probably be here by midnight, yay! Less than 24 hours labor!” to “I’ve got to push it out right now?! HERE?!” I freaked out. And I didn’t want to tear so I didn’t want to push. So I let my body just push and while she was right there I knew if I gave it a little umpf she’d come out but I didn’t want to. Instead….I screamed and huffed and puffed and arched my back and cried and was way crazier in these few pushing contractions than I was in 4 hours of pushing out Stella.

Ollie tried to tell me how to be more productive so I’d stop freaking out and just screaming through it and actually try to get the baby out. Her heart tones were fine but there was meconium. Tony was a mix of emotion, cheerleader and helper. He watched it all. I felt the head coming down. It was hard and I didn’t want it to be there, I wanted to be done. I felt the crowning. When the crowning started I decided I was done and I bared down hard and popped her head out. I asked if the whole head was out, I could see most of it and it was. The midwife checked to see if there was a cord around her neck and there wasn’t. I waited for the next contraction and pushed her shoulders out. There was a little resistance and I didn’t feel that 1 shoulder, 2nd shoulder delivery that I felt with Stella. I pushed out her shoulders at one time then the rest of her just shot out along with a TON of water. The midwife suctioned her since there was meconium in the water but as soon as she was done I was bringing her to my chest. I pushed for maybe 20 minutes max. During pushing our assistant midwife showed up. I just looked over and said hey to her and smiled at one point. She was born at 4:45pm


Tony and I were both in the aw and oh my God that just happened state. It was a GIRL! And she wasn’t huge. She was covered in vernix which was another first. My placenta took about 45 minutes to come out. I was really over that. The contractions were uncomfortable and I just wanted it out. I pushed out about 7-8 tangerine sized clots. Actually, I shot them out and we thought it was the placenta until that happened. Finally it came out and I was much much better. It was nice to not have a retained placenta like I did last time! I felt great right away. The baby nursed for a solid 20 minutes. I took a shower and put on clean clothes and the midwives cleaned up and changed the sheets. Tony held the baby while I showered and just stared at her. Once cleaned up we ate and they did the newborn exam. She checked out perfectly. Graham and Stella were in and out once the baby was born. They didn’t come in during pushing, I’m sure it was scary, I was pretty loud but they did come up when it was over. We realized it was still early evening and decided they should go to school the next day so we made sure they ate dinner and got ready for bed. They both seemed ok with what they heard and saw.
After all was settled it was just the three of us, Papa, Mama and baby. We stared at her and talked about what happened. Tony slept a good bit. I dozed here and there. We woke up this morning and made sure the kids were ok, spent some time with them in our room with the baby and then saw them off to school. I hardly feel like I had a baby. I didn’t tear at all. I’m a little tired and a little sore but otherwise fine. We had some confusion about her birth weight but after re-weighing twice she was 7lbs 12oz, 20.5 inches long and 13.75 inch head. She was a full pound and a half smaller than my first VBAC baby, almost 2 inches shorter and head 1.75 inches smaller diameter. I had her 12 days earlier than the last one too. I went from a 40 hour labor with 4 hours pushing to 8 hours and about 20 minutes of pushing. It’s amazing how different I feel. I totally had a business hour baby!!








Read Full Post | Make a Comment ( 1 so far )


